
Feet Also Need Cosmetic/ Plastic Surgery for Good Looks (A New Perspective) World’s First, Graded, Mega Skin Expansion by Fusion 4-In-1, Correcting, All-Inclusive, Extreme Clubfoot Deformities- A Game Changer
Rattan L. Mittal*
Emeritus Professor, Orthopaedic Department, GOMCO, Patiala, India
Abstract
Introduction: Congenital clubfoot, the commonest orthopaedic defect and with very high prevalence rate in LMICs with tremendous GBD (80% global population), still remains unsolved, with 95% relapses/ under-corrections, in extreme deformities (Mittal1), besides the umpteen uncorrected deformities. Author has researched this unexplored area for over fifty years, still continuing. AIM: Cosmetology/ Plastic surgery are the deep routed foundations of this high rise, evidence based, research. Being need based, it was destined to happen in three phases. This is, FIRST EVER, successful use of the four popular plastic procedures in a single incision1 (Rotation, Z-plasty, vY-plasty and Fillet flaps), nicknamed as FUSION 4-in1, by any surgeon (including plastic and orthopaedic surgeons) on any part of HUMAN BODY, leave aside CLUBFOOT. This is A LOUD AWARENESS CALL for improving looks, function and avoiding complications.
Methods: These were need based, 3 phased, persistent, sequential endeavors: PHASE 1, the anatomical dissections2 and years of clinical observations, leading to discovery of heterogeneous 3D skin contractures (foot being a 3D organ) as the reason for all failures. Rotation flap was used for the first time in CLUBFOOT for correcting grade 1 of this deformity with an authentic publication of a series of one hundred cases documented in SICOT JOURNAL (Mittal)3. With a thumbs-up start, it progressed to higher evolutionary stage of PHASE 2, in more extreme deformities: combining Z- plasties (1, 2 or even 3 Zs) with rotation flap as 2-in-1 incision and then to PHASE 3 for even more rigid deformities, adding VY-plasty also with rotation + Z-plasty, as 3-in-1 incision and even adding fillet flap as 4-in-1 in a lone OCTOPUS CLUBFOOT, World’s first case. RESULTS and CONCLUSIONS: The Triple or even Tetra skin expanding incision gave consistently gratifying results with longer, flexible, better functioning and pleasing looking feet, with long term follow up as reported and published in a Landmark SICOT publication of 1080 cases over a 40 years period with a long term follow up averaging 12½ years (Mittal)1.
Cosmetology and plastic surgery, in this evidence based, cutting edge research, achieved the distinction of, FIRST EVER use of the 4 procedures in a single incision transforming “CROOKED TO ROZY FEET”. ROZY is an acronym and stands for ROtation, Z-plasty and vY-plasty (Mittal)4. This is also a LOUD Awakening Call to disseminate this surgical concept for correcting the more rigid and severe deformities, with relapses and under-corrections at any age, including the uncorrected ones for the Global clubfoot community.
Background
Destiny is inevitable. “TRUTH IS STRANGER THAN FICTION” and it has to be, because FICTION is the creation of human mind and under its control, but TRUTH just happens of its own with no control. This CLUBFOOT RESEARCH has proved its veracity once again.
BELIEVE IT OR NOT! This lifetime research started more than 50 years ago, was destined to happen, that too at Patiala and reach its pinnacle. The very first decision of moving to Delhi after graduation in medicine, in January 1961, proved to be a clincher. There have been many sequential events since then, one after another, in perfect order, happening till now. Details of all these have been highlighted in the PREFACE and INTRODUCTION of author’s world-class, invited, COMPREHENSIVE BOOK ON CLUBFOOT, ISBN:9781138083738, published by Taylor and Francis. This is a premier Global publisher, (Informa Group, London, UK) and this book in now available worldwide on Google search.
Incredible, Sequential Repetition of Number 3, Time and Again
1. Anatomical dissection of 15 clubfeet in stillborn fetuses (15/ 5 = 3).
2. Three phases of this need based research.
3. Three plastic surgery procedures usage.
4. Fusion as 3-in-1 incision- Triple surgical skin expanding incision,
5. First ever, all three original research awards of Indian Orthopaedic Association: Silver jubilee in 1988, Golden in 2013 and Diamond in 2108.
6. Three U-TURNS to Government Medical College Patiala for this research from outstations, 1st time from Delhi; India’s Capital 1961, 2nd time from Rohtak (Haryana State) in 1964 and third time in 2018, appointed as Emeritus Professor at Govt. Medical College Patiala, 23 years post retirement, to contribute to research, academics and poor free clubfoot surgeries.
7. Three honours at Coimbatore in 2018 (Tamil Nadu IINDIA): i. comprehensive lecture on this research; ii. Diamond Jubilee Award and iii. CLUBFOOT BOOK Release on 29th November at 2018 annual IOACON
8. Date of Book release: 29 + 11 + 2+0+1+8 =51 or 5+1 = 6/2 = 3.
9. I have performed at GOMCO Patiala, as Emeritus Professor, a poor free, twice relapsed grade 3 deformity, by triple skin expansion (3-in-1) clubfoot surgery on a 17 years old female patient on 21st September 2019, with pre-op teaching class and live demonstration of 3½ hours surgery to orthopaedic department staff (2+1+9+2+0+1+9 = 24/8 = 3).
10. Date of marriage 26.2.1967 (2+6+2+1+9+6+7= 33/11=3), a renowned Dermatologist, also a Dr. B.C.Roy National Awardee, a great motive force.
11. I have three daughters and 3 grand-daughters helping me in this great adventure.
Facial Versus Pedal
Looks
Since time immemorial, facial looks had always received the prime attention, world over, by cosmetologists and plastic surgeons than any other part of human body. CLUBFOOT is the commonest orthopaedic deformity and the severer neglected deformities (many subgroups), lead to numerous handicaps, with no satisfactory solution available before this research. With the newer surgical concepts, invented by the author in this research, highly satisfying solutions are now possible for all such deformities, rarest of rare, at all ages. Time has come, when foot should be given preference over face due to many reasons given below:
Importance of feet
Without feet, humans could live only vegetative life. Deformed feet lead to enormous psycho-physico-socio-economic handicap. Feet are an organ of locomotion, for day to day living and earning livelihood. If the feet are deformed, the above functions are bound to suffer, besides the psychological effect of unsightly looks e.g. More the deformity, more will be the handicap. Innumerable early and delayed complications will occur as time passes, actually seen by the author, as listed in my publications. As an example of a social handicap is not getting a good life partner and this becomes a reason for surgery (Figures 10 and 11) Therefore, if given to choose one, author feels, choice will invariably fall on getting the healthy good looking feet first, rather than good looking face. Face will be a second choice.
In INDIA, feet are important for other reasons too: we bow to the feet of our DIETIES, teachers and all elders, which can be embarrassing with deformed feet. This act brings humility, an important ingredient for a positive attitude in life. There are umpteen popular INDIAN DANCES from various parts for the women folk. Female folk have special jewelry, henna colouring for the feet to improve looks. Even in western countries, high heels footwear, are high in fashion and one cannot dream of it with clubfoot deformity. With deformity corrected, all these things will become meaningful.
Cosmetology and Plastic Surgery as Related to Clubfoot
They are the foundations of this, unparalleled, research and enlarging the contracted fascio-cutaneous chamber, to have orderly layout of tightly packed contents, is the first thing to do for achieving worthwhile deeper correction. This research is now unending due to another discovery, that ”EACH CLUBFOOT IS DIFFERENT”. However, these techniques are not just treatment for any particular case, but unbeatable surgical concept for any case and transforming every CROOKED CLUBFOOT to ROZY FOOT with pleasing looks. ROZY (sounds same as rosy) is an acronym derived from the technical names of plastic surgery procedures: RO stands for ROtation skin flap (1st phase of research), Z stands for incorporated Z-plasty in rotation flap (2nd phase) as 2-in-1 and Y for added vY-plasty in the first two (3rd phase), making it a 3-in-1 technique. In a, world’s first, the most extreme deformity with triple axes rotation and many other birth defects, with a new name of OCTOPUS CLUBFOOT, fillet flap was also added to the above three procedures, as 4-in-1 achieving excellent result. This case is viral on Google search.
Incidence, an Unsolved Global problem
Clubfoot is the commonest congenital orthopaedic defect, highly prevalent in LMICs with 80% of Global population and still remains unsolved. This is especially true of more rigid and neglected deformities, reported in literature with scores of confusing names e.g. neglected, recurrent, relapsed, residual, resistant, recalcitrant, severe, rigid, syndromic, isolated, from child to adults and up to 95 percent failures (Tarraf and Carroll)5. Besides that, umpteen cases remain uncorrected till late age due to TABOO and poverty, commonly seen in LMICs. Millions of DALYs are wasted world-wide with tremendous GBD (Ponseti 20066). There has been lack of commitment for research in this global Problem of the poor clubfoot community living with psycho-physico-socio-economic handicap. All the contemporary techniques were good for mild and moderate deformities. The more rigid grade 3 deformities defied corrections and resulted in mass failures as reported in literature, skin contracture always remained neglected.
Present Research
Author has been researching in this unexplored grey area, since more than 50 years and a generic name of TRIMORPHIC (3 grades) EXTREME DEFORMITIES has been given to all of them, because of their common aim of good correction. This research has been accomplished in need based, THREE PHASES:
FIRST PHASE continued for about 25 years in grade 1 deformities in two stages: 1ST STAGE was study of patho-anatomy in 15 clubfeet of stillborn fetuses. Postero-medial Skin contracture in 3D was discovered as the most important primary cause (Fig.1) of all failures (Mittal etal 1981)2. This discovery was reinforced by years of clinical observations. It was conceived that deeper patho-anatomy could only be corrected if the fascio-cutaneous container was enlarged in 3D by a Dorsolateral skin flap rotated postero-medially. The 2ND STAGE of phase 1, to prove the above hypothesis, was a clinical study of 100 cases of GRADE 1 extreme deformities, successfully corrected by enlarging the skin pouch in 3D by a DOrso-LAteral Rotation skin flap. This was published in International Orthopaedics (SICOT)3.
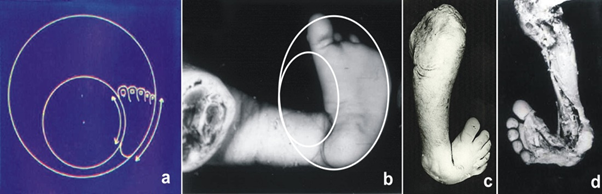
Figure 1: A Simulated 2 circle diagram on clubfoot cadaver specimen showing skin Contracture on single medial plane and this contracture is in 3D. the second Cadaver also shows similar skin and deeper pathoanatomy. (With kind courtesy taken from author’s clubfoot book Taylor and Francis ISBN:9781138083738)
Then started the 2ND PHASE, a need based project, because more rigid deformities (grade 2) started coming for treatment, which needed more extensive skin expansion. Therefore, Z-plasty was also added in the Rotation flap successfully, as 2-in-1, and continued for about 15 years. This too was published (Mittal 2014)6.
The THIRD PHASE, the most significant and also need based, because even more rigid; grade 3 extreme deformities started presenting for treatment. Author got many periodic awards/ rewards, motivating to continue. NECESSITY IS THE MOTHER OF INVENTION” is a well-known saying. After the FIRST PHASE and facing more severe deformities requiring more fascio-cutaneous room for good correction, a newer approach was required.
Third phase research has been going on since more than 5 years now, mostly as FUSION 3-in-1 incision. Author has accomplished first ever use of all 3 plastic surgery procedures in one incision, by any surgeon as 3-in-1 and even 4th procedure, the FILLET FLAP also in the same incision, as 4-in-1, in one case. This lone case in point is OCTOPUS CLUBFOOT, world’s first case, by quadruple 3D skin expansion. This case is documented, In International Orthopaedics (SICOT) Journal1 in Table No 1 and also in my Clubfoot Book as above. This, being the first, evidence based, MEGA 3D SKIN EXPANSION, by FUSION: 4-in-1 incision, needs to be highlighted for its immense value, because this led to the discovery of these techniques as an innovative surgical concept (Mittal 2018)4 for rarest of rare, all inclusive, even the most rigid deformity.
Other variants of plastic procedures used: Quite often, in more rigid deformities, many other cutaneous plastic surgery procedures have been done: Thiersch grafts for minor skin defects, double VY-plasties: either side by side or one above and other below; circular Z-plasties in Congenital constriction bands in 4 sections, one or more lazy z or V to lengthen skin, proximal relaxing incision, additional medial VY-plasty to correct hallux varus, or dorsal one to correct hyperextended toes or plantar one to correct plantar-contracture of toes. All these are required for correction of deformities, to maintain collateral circulation and consequently to improve the looks of the foot.
Each Clubfoot is Different
The third phase research, also opened floodgates for unlimited further research in clubfoot, because of an important discovery that every clubfoot is different with different patho-anatomy, which has been proved on ample evidence, details given in SICOT publication and Clubfoot Book1,7. Their description is beyond the scope of this journal, being detailed issues.
Author received numerous periodic Awards and Rewards. Latest ones are: 1. Due to my expertise and special authorization in 2016-17, under Govt. of India’s National Health Mission program, I performed, a record, 38 poor free, unique, Clubfoot Surgeries at Govt. Mata Kaushalya Hospital Patiala. Many of them adore author’s CLUBFOOT BOOK and many figures in this article are from those cases. World first, OCTOPUS CLUBFOOT, viral on Google, is also one of them; 2. An invited lecture at Global Foot/ Ankle Congress at Chongqing. China May 2017; 3. Publication of a comprehensive article in International Orthopedics, SICOT8, in June 2018 issue at DOI 10.1007/s00264-017-3741-6; 4. An invited BOOK7, written and published for Taylor and Francis, a premier Global Publisher Informa group London U.K, released on 29th Nov. 2018 at Annual IOACON at Coimbatore with 7000 delegates including over a 1000 from oversea, ISBN No 9781138083738. This is available world over, at more than 125 sites, on Google Search and list is expanding with time and 5. Appointed Emeritus Professor Govt. Medical College Patiala India for promoting research, academics and poor free surgeries and I performed the first successful poor free, 3-in-1, 3½ hours unique surgery without fusion in a 17 years female, with double relapse after earlier surgeries, having a real ugly looking foot.
Results/ Conclusions
Results were graded on the basis of patient satisfaction, because patient is the best judge in view of every clubfoot being different. The results as published in 2018 SICOT publication, in 800 feet, with long term follow up of average 12½ years, out of 1080 surgeries: They were 96 % excellent/ good with satisfied patients and fair/ poor only in 4 %. The results were highly gratifying with longer, flexible foot with pleasing looks.
Discussion
Heterogeneous skin contracture in 3D has been considered as the most important hindrance in achieving a good acceptable correction in extreme (as defined above) deformities. The varied contractures may be only congenital in nature or may be additionally complicated by varied scars of previous one or more surgeries. Unless the room is bigger, everything will have to be squeezed in tightly with no breathing space.
Therefore, skin chamber will have to be enlarged in 3D, as contracture is also in 3D, foot being a 3D organ. The amount of expansion of skin container will also vary depending upon the degree of contracture. Author invented Triple Surgical Skin expanding skin incision in, need and evidence based, 3 phases; initially as single, then 2-in-1, and finally as 3-in-1 and even 4-in-1 in a lone, Octopus Clubfoot, a new entity. Solid abundant evidence has been derived from the study of numerous National and International plastic surgery journal articles. Bhattacharya’s pioneering articles9-21 were of immense value in the present context. Cadaveric dissections, animal experiments and clinical experience provided the crucial evidence for covering defects. Plentiful vascular and lymphatic microcirculation in the subfascial and suprafascial planes was demonstrated, with myriad perforators originating from all levels from deepest to most superficial planes. Therefore, addition of one or more Z-plasties as in 2nd phase and later on, even VY-plasties, as in 3rd phase could be done with full confidence with a meticulous dissection. However, remaining superficial to suprafascial plane avoiding injury to perforators for maintaining continuity of fascia with skin, is imperative for success. In vY-plasties, DISTAL BASED ISLAND FLAPS OF VARIOUS SIZES could be designed to cover varied gaps in ankle area in the same incision, to maintain vascular continuity, the lifeline of the flaps. There are about a dozen more skin procedures, as listed above, which may have to be used, as need based, to correct the varied kaleidoscopic contractures and maintain vascularity. There may occasionally be superficial marginal necrosis, but due to tremendous network of collaterals, correction of deformity is not affected. Deeper correction, also varied in character, could only be possible, if fasciocutaneous chamber has been adequately enlarged.
Innumerable unusual complications were encountered as indication for surgeries and treated by the author, which are beyond the scope of this journal but can be seen in the author’s clubfoot book. In fact, these surgical techniques are a surgical concept for treating even the most rigid deformity. This fact was discovered after correcting OCTOPUS CLUBFOOT by the first ever 4-in-1 incision, the most rigid deformity to date and published by the author4.
Cosmetology and plastic surgery have been the backbone of this research to give the patient a longer, flexible foot, without arthrodesis, pleasing looks and better functioning on long term. Combined use of all the four plastic surgery skin procedures in a single incision, i.e. DOrsoLAteral Rotation skin flap, Z-plasty, vY-plasty and Fillet flap (FUSION 4-in-1) have been successfully accomplished for the first time by any surgeon. This has been a need based 3 phase research, acronymic as: DOLAR in phase 1, DOLARZ in phase 2 and DOLARZ-E (E means Extended) in phase 3. These 4 plastic surgery procedures improve the cosmesis of the foot also to a great extent, besides much better function. Use of numerous other skin procedures, varied due to varied skin patho-anatomy and will go on varying due to differences in each foot.
Assessment criteria were based upon patient satisfaction, because of the evidence based discovery7,8 that “Each clubfoot is different” and no contemporary criteria system could be applicable. Transforming ugly looking foot, to give a pleasing ROZY (sounds like rosy) looks, has been an important ingredient of satisfaction. ROZY is an acronym, derived from: ROtation, Z-plasty and vY-plasty, the main words in the triple techniques.
To Conclude, author’s contribution: The main purpose of this publication is to highlight the message globally, giving it wings, that FEET also need good pleasing looks for many reasons cited above. Besides the looks, feet are an organ of locomotion, for day to day living and enabling man to earn livelihood. By this new surgical concept of triple or even tetra surgical skin expansion with highly satisfying results, saving millions of wasted DALYs and enormous GBD with psycho-physico-socio-economic handicap to the patients. Cosmetology and plastic surgery in the present form, the first ever, can become a boon. The unfortunate global clubfoot community of LMICs, with extreme deformities, requires a total commitment and dedication of the operating surgeon. Besides, occasional inconsequential marginal necrosis, the only limitation of these all-inclusive versatile surgical techniques that feet cannot become absolutely normal radiologically, functionally of course they can.
Solutions Suggested
1. Author’s SICOT 2018 comprehensive article and the Comprehensive Clubfoot book describe different surgical technique of this surgical concept in a variety of cases for learning purposes; 2. Appointment as Emeritus professor is also going to serve the same purpose of teaching and live demonstrations; 3; I sent suggestions on Google search at their website to Rotary International doing clubfoot work in Africa (disease prevalent) by Ponseti’s casting. This is good for mild and moderate deformities started earliest after birth. otherwise face relapses commonly. Ponseti himself has committed this in his manual and other publications as given in author’s book. There are lots of extreme deformities there requiring these surgeries; 4. I can organize workshops at Patiala in collaboration worth any volunteers. I am an octogenarian passionate researcher and do not travel alone.
To conclude, this is a CLARION CALL, through this article: let only hundred committed plastic/ orthopaedic surgeons come forward for this meticulous surgical work to bring about a visible change in the Global thinking about this deformity. Clubfoot Community is looking expectantly towards us. God bless us all with positive thoughts.

Figure 2: 1Y, M, grade 3, distal plantar skin contracture absent mid-metatarsals, 3 stage correction. 1st stage rotation flap, 2nd stage by VY-plasty of plantar fascio-cutaneous tissues with an innovative soft tissue distractor. 3rd stage (not shown) by plantar VY-plasty of 4th toe skin contracture.

Figure 3: 1â Y, M, B/L deformities, deep CCBs/ amputations, circular Z-plasties from front and back, corrected and walking with an extension prosthesis on right side. Left corrected by Rotation flap (residual adduction).

Figure 4: 2½Y, grade 3 B/L. Excellent correction by 3-in-1 plastic surgery procedures at follow up.

Figure 5: 6Y, F, with CCBs and, Grade 3 right foot and broad CCB, relapsed after previous surgery with calcaneovarus and painful callosity. Corrected by 3-in-1 technique. Callosity also healed at follow up.

Figure 6: 7Y, F, grade3 extreme deformities, walking, on vertical talar head. big callosities 3-in-1, excellent correction.

Figure 7: 13Y, M, grade3, relapse after heel cord tenotomies. 3-in-1 skin expansion. excellent correction.

Figure 8: 15Y, M, grade 3 extreme deformities B/L, 3 earlier surgeries scars-Bow String. Corrected by 3-in-1 (double Z-plasties). Excellent correction.

Figure 9: 18y, F, Grade 3, Octopus Clubfoot (real Octopus). Correction by 4-in-1 (filleted excess bones). Excellent correction, except hypoplasis of whole limb 2½ inches shortening, which can also be lengthening.

Figure 10: 10 and 11: two adults grade 1 unsightly looks, marital problems. Left one relapse with compensatory symptomatic genu recurvatum due to equinus, 1st phase Rotation flap corrected both foot as well as knee.
Right side, 23 yrs M, HIGH DOME grade 1, marital prob;lem. Corrected by Rotation flap phase 1 technique.

Figure 12: 19Y, M, grade 3. Corrected by 3-in-1. Excellent shape with ROZY FEET (good looks).

Figure 13: 22Y, M, extreme grade3, relapse after 2 surgeries, double Z-plasties and rotation flap. Excellent correction right foot.

Figure 14: 45Y, M, grade 3 deformity, crush injury 20 led to healing with scars and recurrent ulcer outer side.
3-in-1 and a unique side by side double VY plasties (one with base down and other with base up. Excellent correction at 1½ years follow up.

Figure 15: 24 Y, M, Grade 2, marked metatarsus + hallux varus, under-correction/ relapse after 2 previous surgeries with old scars. Rotation+ Z-plasty (2-in-1) and another.
Distal VY-plasty to correct Hallux varus. Excellent correction.
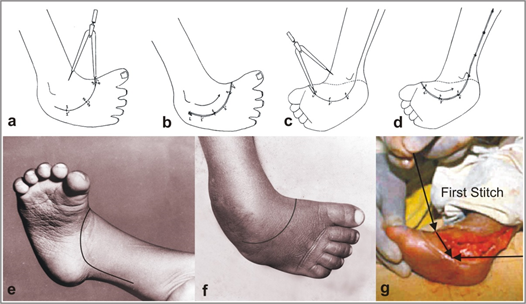
Figure 16A: Description Copied from Fig. 5.1 from Author’s Clubfoot Book: Diagram a - d showing the skin flap marked out with the help of dividers and the amount of rotation at the end of operation. a- Dorsal surface with incision mark; b- Dorsal surface with the rotated flap and arrow showing the direction of rotation. c-Medial and planter side of foot with incision mark; The dog ear on the distal side of skin on dorsolateral aspect is corrected during wound closure; d- Medial and plantar aspect of foot after rotation of flap and wound closure with arrow depicting the direction of rotation and the numbers showing the amount of rotation achieved. e- Incision mark on the posteromedial aspect of a rigid clubfoot in a one year old child. f- Incision mark on the dorsolateral aspect. G.- Application of first stitch and the amount of rotation of the skin flap which can be brought about. Use of dividers was needed in the initial stages of this technique for circular marking on the dorsum with medial side of foot. Later on with experience you can do with a free hand, directly with knife.

Figure 16B: Enlarged Fig. 12 middle picture with ROtation+2Z-plasties

Figure 16C: Showing magnifies view of Fig 9: ROtation+Z+VY+Fillet flap
(4-in-1). K-wire can be seen in the corrected hallux varus at its tip. In the inset there are part of filleted jointed extra toes, WORLD’s First Exotic, most extreme deformity, named OCTOPUS CLUBFOOT.
Self-explanatory Photographs of some patients from 1-45 years age, showing plastic surgery procedures, for good looks and function (ROZY FEET), mostly 3-in-1, but 4-in-1 in one case for good looks and function with highly satisfying results on long term.
Abbreviations: figures: Fig. – figure, Y – year, M- male, F – female, B/L- bilateral, CCBs – congenital constriction bands.
Acknowledgments: This is a review article and its text and large number of figures, from place to place, are reprinted/ adapted by kind courtesy: Springer Nature and Copyright clearance center of Rights Link. From author’s own published articles1-4,7,9.
Kind Courtesy of Taylor and Francis group (CRS Press), a premier Global publisher and adopted from author’s own book Clubfoot-A comprehensive approach (past present and future): 1st edition, by Mittal RL, ISBN;9781138083738. All are duly quoted in the text of this publication.
References
- Mittal RL. Trimorphic Extreme Clubfoot Deformities and Their Management by Triple Surgical Skin Expanders- DOLAR DOLARZ and DOLARZ-E (Evidence based Mega corrections without arthrodesis. International Orthopaedics (SICOT) Online First in Feb 2018 and print version in June 2018; 42(6): 1297- 1306. https://doi.org/10.1007/s00264-
- Mittal RL, Makhni SS, Sidhu GS. Morbid Anatomy of Congenital Clubfoot. Ind J Orthop. 1981; 15: 129-135.
- Mittal RL. The Surgical Management of Resistant Clubfoot by Rotation Skin Flap and Extensive Soft Tissue Release. Int Orthop. 1987; 11(3): 189-92. PMID:3623754, DOI:https://doi.org/10.1007/BF00271446.
- Mittal RL. Octopus Clubfoot Rediscovered - World’s First Exotic Case - A Neglected, Triple Axes Rotational, Grade 3 Extreme Deformity: Corrected by, Unparalleled, 4-In-1 Mega Surgical Skin Expansion from Crooked to ROZY Foot. Ortho Res Online J. 6(1). OPROJ.000627.2019. DOI: 0.31031/OPROJ.2019.06.000627
- Tarraf YN, Carroll NC. Analysis of the Components of Residual Deformity in Clubfeet Presenting for Reoperation. Jour of Pediat. Orthop. 1992; 12: 207-216. http://dx.doi.org/10.1097/01241398-199203000-00011.
- Ponseti IV. Treatment of the Complex Idiopathic Clubfoot. Clin Orthop Relat Res. 2006; 451: 171–176.
- Mittal RL. CLUBFOOT - A Comprehensive Approach (Past, Present and Future); 1st Edition Dec 2018; 198 pages, 45 illustrations. Taylor and Francis (CRS Press), USA. ISBN No 9781138083738.
- Bhattacharya V, Agrawal NK, Chaudhary GR, et al. CT Angiographic Evaluation of Perforators in the Lower Limb and Their Reconstructive I0mplication. IJPS. 2012; 45: 494-497.
- Mittal RL. Obstinate Clubfoot with Triple Plus Dislocation. J Foot Ankle Surg (Asia-Pacific). 2014; 1(2): 72-77.
- Bhattacharya V. Experimental and Clinical Evidence Based Rationality of Incorporation of Deep Fascia in Tissue Transfer for Reconstructive Surgery. Ann Natl Acad Med Sci (India). 2016; 52(4): 222-231.
- Ponten B. The Fasciocutaneous Flap its Use in Soft Tissue Defects of Lower Leg. BJPS. 1981; 34: 215- 220. DOI:10.1016/s0007-1226(81)80097-5.
- Cormack GG, Lamberty BGH. The Fasciocutaneous System of Vessels. The Arterial Anatomy of Skin Flap. Churchill Livingstone. 1986.
- Taylor GI, Palmer JH. The vascular Territories Angiosomes of the Body Experimental Study and Clinical Applications. BJPS. 1987; 40: 113- 141. DOI:10.1016/0007-1226(87)90185-8
- Bhattacharya V, Deshpande SB, Watts RK, etal. Measurement of Perfusion Pressure Perforators and its Correlation with their Internal Diameter. BJPS. 2005; 58: 759-764.
- Bhattacharya V, Watts RK, Reddy GR. Live Demonstration of Microcirculation in the Deep Fascia and its Implication. Plast Reconstr Surg. 2005;115: 458-463.
- Bhattacharya V, Goyal S. A Dye Study in Fresh Cadavers to Outline Retrograde Flaps of the Lower Limb and to Examine Clinical Implications. Europe Journ of Plast Surg. 2006; 28: 458-463.
- Bhattachatya V, Goyal S, Jain P, et al. Angiographic Evaluation of Fasciocutaneous Flaps. Int Surgery. 2006; 91: 326-331.
- Bhattacharya V, Reddy GR, Goyal S, et al. Skeletonised Retrograde Distal Perforator Island Fasciocutaneous Flaps for Leg and Foot Defects. J Plast Reconstr Aesthet Surg. 2007; 60: 892-897.
- Bhattacharya V, Reddy GR, Goyal S, et al. Skeletonised Retrograde Distal Perforator Island Fasciocutaneous Flaps for Leg and Foot Defects. J Plast Reconstr Aesthet Surg. 2007; 60: 892-897.
- Bhattacharya V, Barooah PS, Nag TC , e t al . Detailed Microscopic Analysis of Deep Fasciaof Lower Limb and its Surgical Implication. IJPS. 2010; 43: 135-140.
- Bhattacharya V, Choudhuri GR, Mishra B, et al. Demonstration of Live Lymphatic Circulation in the Deep Fascia and its Implication. Europe Journ of Plastic Surg. 2011; 34(2): 99-102.