
Racial and Ethnic Disparities in Androgenetic Alopecia Clinical Trials in the United States
Ishita Aggarwal BA; Carolina Puyana MD, MSPH*; Neha Chandan MD, MPH; Roger Haber, MD
University of Illinois at Chicago, Department of Dermatology, 1801 W. Taylor St., Chicago, IL 60612-7307
Abstract
Introduction: Androgenetic alopecia (AGA) is the most common type of hair loss worldwide and is estimated to affect about 80 million people in the United States. Recent trends suggest that incidence and severity of the disease are increasing across all genders and races. Randomized controlled trials (RCTs) involving diverse patient populations are necessary to individualize treatment.
Objective: Evaluate enrollment and subgroup analysis of people falling in racial/ethnic minority groups in phase II and III RCTs for AGA published in the United States within the past 10 years.
Methods: We examined completed published phase II and III randomized, double-blind, placebo-controlled trials investigating AGA. Race/ethnicity data was extracted for each RCT using US Census Bureau guidelines.
Results: 20 total RCTs with a total of 1855 participants were included in the analysis. 8 (40%) of RCTs included race/ethnicity data. Among these, 3 (15%) studies included only race and 5 (25%) included both. The majority of study patients were white (n= 862/1063, 81.1%) followed by African American (n=127/1063, 11.9%) and Asian (n=33/1063, 3.1%). Six (0.56%) patients identified as American Indian/Alaska Natives, 5 (0.47%) as Hawaiian/Pacific Islander, and 16 (1.5%) as another race or race was unknown. Ethnicity was reported in 5 (25%) of trials, totaling 317 participants; 60 (18.9%) patients identified as Hispanic.
Conclusions: Non-Caucasian patients remain underrepresented in RCTs despite AGA being a highly prevalent condition, reducing the generalizability of trial outcomes to the general population. Future RCTs should update definitions of race/ethnicity and include more diversity among AGA patients.
Androgenetic alopecia (AGA) is the most common type of hair loss worldwide, estimated to affect about 50 million men and 30 million women in the United States (US)1,2. AGA is thought to be genetically predetermined with variable penetrance2,3. Furthermore, both incidence, severity, and patterns of hair loss appear to differ across different racial and ethnic groups3. Recent trends suggest that incidence and severity of the disease are increasing across all genders and races. Thus, randomized controlled trials (RCTs) involving diverse patient populations are necessary to further understand how we can personalize treatment for patients.
We evaluated enrollment and subgroup analysis of people falling in racial and ethnic minorities in published phase II and III double-blind RCTs investigating AGA performed in the US within the past 10 years. Search term “androgenetic alopecia” was queried of ClinicalTrials.gov and PubMed following the selection process depicted in figure 1.
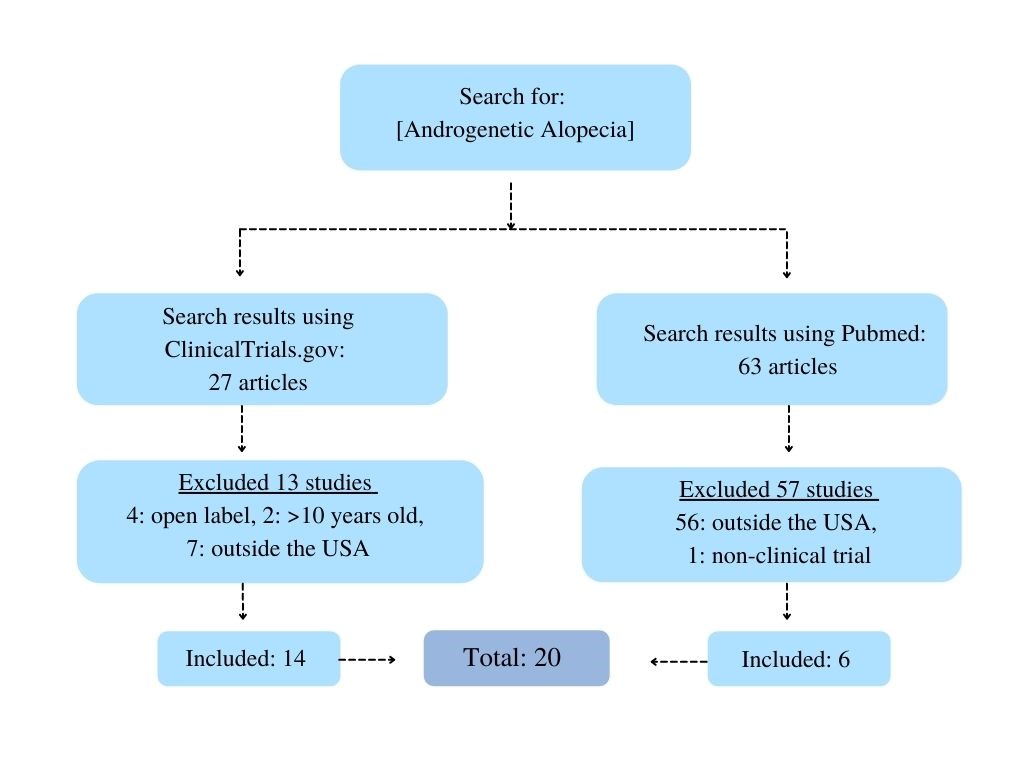
Figure 1: Androgenetic Alopecia, search methodology and results of the review
Race and ethnicity data were extracted for each RCT using the definitions outlined by the US Census Bureau5. Race represents an individual’s self-identification in one or more groups including White, Black, African American, American Indian or Alaska Native, Asian, and Native Hawaiian or other Pacific Islander, or another race. Ethnicity refers to being of Hispanic or non-Hispanic origin.
20 total RCTs were included in the analysis for a total of 1855 participants. 8 (40%) were published within the last 5 years (2018-2022) while a majority (60%) were published between 2012 and 2017. 8 (40%) RCTs included race and/or ethnicity data, accounting for 1063 patients. Among these, 3 (15%) studies included race but not ethnicity and 5 (25%) included both. White patients accounted for most study participants (n= 862, 81.1%) followed by AA (n=127, 11.9%) and Asian (n=33, 3.1%) patients. Six (0.56%) as American Indian or Alaska Natives, 5 (0.47%) patients identified as Hawaiian or Pacific Islander, and 16 (1.5%) were either identified as another race or race was unknown. The categorization of subject race is shown in figure 2. Ethnicity was reported in 5 (25%) of trials which included a total of 317 participants. Of these, only 60 (18.9%) patients identified as Hispanic.
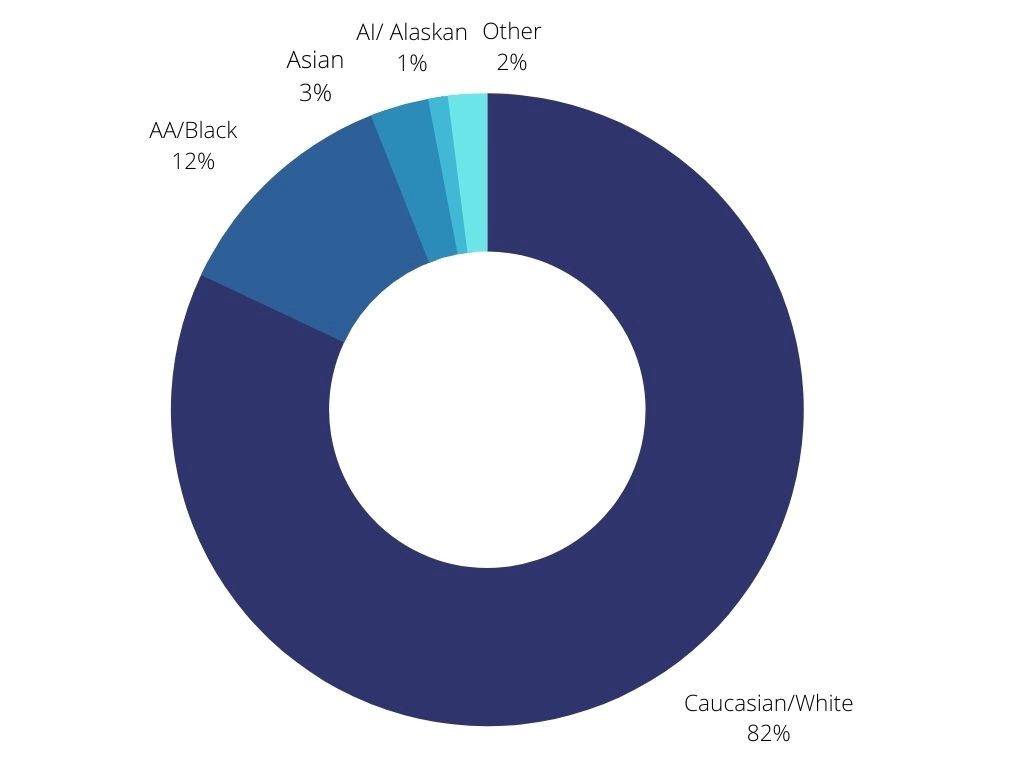
Figure 2: Androgenetic Alopecia: categorization of race in clinical trials in the USA published between 2012-2022
Limitations of this study include incomplete reporting of race and ethnicity, and the use of the broad definition outlined by the US Census Bureau.
Our analysis demonstrates under-representation of non-Caucasian patients despite AGA being a highly prevalent condition. Epidemiological studies have shown that white patients exhibit the highest incidence and severity of AGA followed by African Americans (AA) and Asians3. Native American and Alaska Native patients are least commonly affected. Patterns of hair loss vary between racial groups, as well, with Caucasian males being less likely to have preservation of their frontal hair lines compared to AA, Asian, and Native American men4. Incidence in Caucasian males is estimated to be 50% by age 50 and up to 80% by age 703. In females, incidence is thought to increase after menopause3. However, there are few clinical trials including patients belonging to most minority racial and ethnic groups and none describing how response to treatment may vary across racial and ethnic groups. This limits the generalizability of treatment and trial outcomes to the general population since incidence, severity, and patterns of hair loss appear to vary across different racial and ethnic groups. By incorporating updated definitions of race and ethnicity and making active efforts include more non-Caucasian patients, we can provide more individualized care to patients with AGA.
Conflicts of Interest: None declared.
References
- Androgenetic alopecia: MedlinePlus Genetics. Accessed March 28, 2022. https://medlineplus.gov/genetics/condition/androgenetic-alopecia/.
- He F, Shen M, Zhao Z, et al. Epidemiology and disease burden of androgenetic alopecia in college freshmen in China: A population-based study. PLOS ONE. 2022;17(2): e0263912. doi: 10.1371/journal.pone.0263912.
- Ho CH, Sood T, Zito PM. Androgenetic Alopecia. In: StatPearls. StatPearls Publishing; 2022. Accessed March 26, 2022. http://www.ncbi.nlm.nih.gov/books/NBK430924/.
- Cranwell W, Sinclair R. Male Androgenetic Alopecia. In: Feingold KR, Anawalt B, Boyce A, et al., eds. Endotext. MDText.com, Inc.; 2000. Accessed March 28, 2022. http://www.ncbi.nlm.nih.gov/books/NBK278957/.
- All About Race and Ethnicity in the Census - MCDC. Accessed March 10, 2022. https://mcdc.missouri.edu/help/race-ethnicity.html.